Students travel to London to compare U.S. and U.K. health care
By Katie Neitz
Continuing debates over health care reform in the U.S. and National Health Service funding in the U.K. made the focus of a short-term study abroad program especially relevant.
Seventeen Lafayette students and two Lehigh students spent eight weeks in London, where they studied differences between health care in the United States and the United Kingdom.
The interdisciplinary program, titled “Ethical, Social, and Economic Issues in Health Care in the U.K. and the U.S.,” provided students the opportunity to participate in seminar discussions, conduct research, and work in a London health care or human services environment.
Chris Ruebeck, associate professor of economics, and Brett Hendrickson, associate professor of religious studies, led the course, which is offered every other year. It was originally launched by Alan Childs, emeritus professor of psychology, and Steve Lammers, emeritus professor of religious studies, in 2005.
Students spent their first three weeks in London taking a seminar-style course, in which they discussed cultural, social, and economic differences between the two health care systems.
“We looked at the history of the two systems, the roles that the government plays in society, and how cultural differences impact how health care is delivered and experienced,” says Hendrickson, who researches religion and healing.
Classroom instruction dovetailed into a four-week internship experience, where students had the opportunity to work in hospitals, research facilities, government agencies, and community organizations. The goal was to have students connect Ruebeck and Hendrickson’s teachings with their own real-world experiences.
Julia Hall ’19, a psychology major, spent her internship working at a refugee center, her first time in such an environment. “It really put things in perspective for me,” she says. “I heard from women how hard it was to get prenatal care, birth control, and mammograms. It was depressing at times, but it made me appreciate all that I have.”
After completion of their internships, students had a final wrap-up week to share and learn from each other’s experiences.
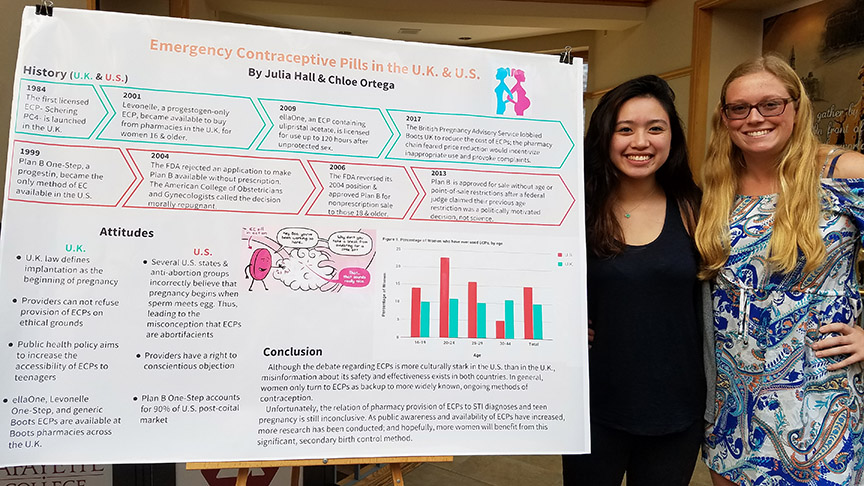
As part of their coursework, students completed a final group research project, which they presented in a poster session on campus in September. Students found stark differences between the two countries as they compared suicide rates, mammogram screenings, cigarette use, and pharmaceutical advertising. For example, greater access to firearms in the U.S. seems to correlate with the higher suicide rate there than in the U.K. And the fact that the U.S. allows direct-consumer advertising of prescription drugs is linked to higher prescription rates in the U.S. versus the U.K.
“It was valuable for me to see how cultural differences really play a role in health care,” says Chloe Ortega ’19, an English and biology double major who is on a pre-med track. “I also learned how important it is to understand legislation as a physician and how it can impact your patients.”
Ruebeck is pleased with what the students were able to accomplish during their time overseas. “For each of these projects, they rose to become an expert, and they did it very quickly,” he says. “We are only there for eight weeks. As is true for Lafayette students, the way they pulled together to deeply investigate their research topics was impressive.”














1 Comment
After graduating from Lafayette in 1969 and directly entering military service overseas in Europe and Vietnam, I determined to get an MBA and begin an international business career in Europe. Senior financial management roles enabled me roughly to evaluate medical systems throughout the continent. But four decades of life in Paris, London, Brussels and Munich gave a far greater appreciation. Of these four lands I found Germany to lead the field (by far), France and Belgium were nearly equal with good care – probably equivalent to quality US care – but England was and remains at the bottom. (My English colleagues who were based in Belgium and I joked that during trips to the UK we should carry letters, requesting that any emergency medical care should be deferred until we could be repatriated to Brussels (or anywhere else in Europe.)) Also, while many pharmaceutical products come from US companies the higher prices in the US versus overseas has much to do with the splintered purchasing power of thousands of smaller health carriers. In Europe there is often one government purchaser for the entire country. Nonetheless, another big difference is that Europeans realize that little is more important than good health and so the higher fees in Germany are linked to ever better care and paid in accordance with earnings. Europeans love their autos as much as people in the US but they gladly run, bike or hike whenever possible and not just for sport but daily activities as well. Lower obesity rates and fewer related illnesses are no surprise.
Comments are closed.